







Much has been touted in the media and social media about the recent proton pump inhibitor (PPI) study in JAMA relating long term use of these drugs to chronic kidney disease. There is so much hype that I thought it important to take a closer look.
The study in JAMA is only available to the public as an abstract, which means the authors condensed an 8 page document into 7 paragraphs (basically a half-page). This is standard…you have to PAY to be able to read the whole article, and the abstract doesn’t tell the whole story. Your old pal, an individual who cares about his listeners, arranged to get a full-text copy of the article so we can go over the “numbahs” together.
First, this is a “cohort study” and it’s “retrospective” and therefore “observational.” This means they took a ton of people who were in another study (Atherosclerosis Risk in Communities (ARiC)) and teased out information they weren’t originally looking for out of the data after the fact. Basically you take 10,000 or more people and find the ones on long term PPIs and see how many developed kidney disease (and how you define that matters) and compare them against all the people in the group who DIDN’T take PPIs and see if there’s a difference. This is a decent study, as far as cohort studies go, but when we look at levels of evidence, we see that this kind of study isn’t the best for proving a scientific point:
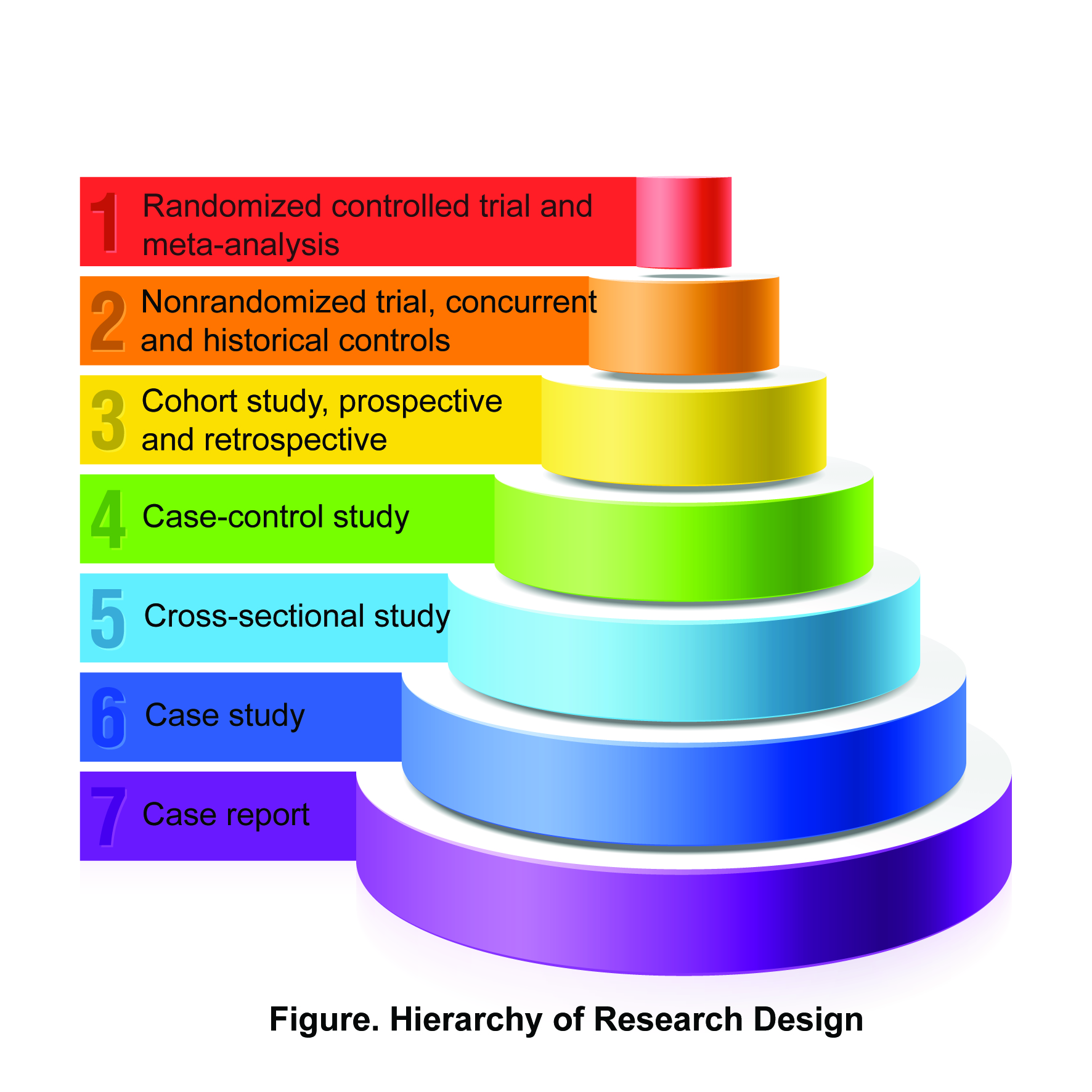
There are two levels of evidence above cohort study that are generally considered to result in better quality, and therefore more believable, results. Performing a double blind, placebo controlled study comparing kidney disease rates in PPI vs Non-PPI users would take another 10 or more years to complete, so this is the best data we have right now (and it’s decent, as I said.) So let’s go with it.
There were 10482 participants in the ARiC study. Since this study was not designed to look at PPI use initially (the data was gathered as part of a general information gathering system regarding the patients enrolled), there were some lopsided aspects to the PPI group. For example, the PPI users were more often obese, white, and hypertensive than the non-PPI users. This is the kind of thing that can cause bias to creep into a study (hypertensive patients are more likely to develop kidney disease, for example) that would be eliminated from a randomized, control trial.
Of the 10482 participants, there were 1438 cases of chronic kidney disease identified (13.7%). There were 56 events in the PPI group (of which there were 322 users), amounting to 17.4% (0.174). In the non-PPI group, 1382 out of 10160 patients developed kidney disease, or 13.6% (0.136). You can spread this out into patient-years and all kinds of things, but we can see that there is a higher percentage of kidney disease in the PPI group than the non-PPI group, and the difference is 17.4/13.6 or a 27.9% increase. (They used another cohort to confirm these results and make the data more powerful.)
This is where the headlines come from: “A 30 PERCENT INCREASE IN KIDNEY DISEASE IN PPI USERS!”
So that certainly seems to be “true,” in the sense that to the best of our knowledge, there is an increased risk of chronic kidney disease in people who take PPIs for years and years, but what does that mean for the individual? And does this make PPIs “bad drugs?”
To figure this out, we need to review the difference between absolute risk and relative risk.
If you have 1000 people in a treatment group and 1000 people in a placebo group, and 10 people have an adverse reaction in the treatment group and only 7 have one in the placebo group, you could say that there is a 30% increase in that adverse reaction in the treatment group. But the ABSOLUTE increase was only 3 patients out of a thousand so the absolute risk to the individual would be 3/1000 or 0.003 or 0.3%. In addition, we can take the inverse of this number to figure out the “Number Needed to Harm(NNH)” (i.e., how many people have to take the drug to have one excess incident of the adverse effect), which in this case would be 333. So the risk to the individual is quite low; your odds would be 332 to 1 of NOT getting the adverse event. Another way to look at it is that 99.7% of the time you’d be ok.
Let’s apply this to the case at hand: The absolute risk of developing chronic kidney disease from taking chronic PPI is 0.174-0.136=0.038. Therefore the Number Needed to Harm is 1/.038, or 26. So the risk to you, the individual, taking a PPI for years and years and years, and developing chronic kidney disease associated with PPI use is 25 to 1, or 3.8%. In other words, you wouldn’t get PPI-associated CKD (assuming this effect is real) 96.2% of the time. We can look at it another way: the risk to the individual is very low, but the risk to society (factor that Number Needed to Harm into the MILLIONS of people taking PPIs every year) is greater. Additionally, this data is from 1996 to 2011, and newer PPIs that were not included may not even have this same effect.
There are other adverse effects from decreasing acid production in the stomach…there may be an increase in bacterial illnesses due to the decrease in bacteria-killing hydrochloric acid in the stomach. There have been suggestions of increased bone fractures in elderly patients who take PPIs chronically, but the NNH is greater than 1200 on that one and may be erroneous.
The flip side of this is that PPIs are very, very effective at what they do. The Number Needed to Treat for total healing of erosive esophagitis is 6. The Number Needed to Treat to reduce GI rebleeding (preventing recurrence after a first GI bleed) is 13. We used to see dozens of vagotomy/antrectomy procedures a year in a decent sized hospital before the advent of H2 blockers (e.g., ranitidine) and PPIs…I believe we saw ONE in our institution last year and that was for someone with a genetic predisposition to overproduction of acid. So PPIs have reduced surgery rates and concomitant surgical complications. In addition, quality of life is improved in patients on PPIs, but only under certain circumstances. PPIs are still “Generally Considered Safe.”
There are adverse effects with every medication (google the number of deaths from acetaminophen last year for an eye opener). Proper medical treatment involves balancing risk vs benefit. Proper medical treatment also dictates that people be treated for the proper indication. It is estimated that 20-70% of people who take PPIs take them without a proper indication. In addition, being OTC, these medications can be taken for years without a healthcare provider’s supervision.
Lifestyle measures may help a significant fraction of heartburn sufferers treat their symptoms without medication. For refractory cases, primary care and gastroenterologists have a full array of treatments, surgical, medical, and lifestyle to relieve symptoms and reduce adverse outcomes. One of the most powerful weapons is still the proton pump inhibitor, so if you’re prescribed one for a proper indication, don’t fear it, just be aware of the risks and benefits and take it only as long as necessary and at the lowest effective dose. Remember, the risk to YOU, the individual is low (but never zero).
yr obt svt,
Dr Steve
